The 4-Hour Bottleneck Test: Does Your Organization Stall When You Step Away?
Systems Guide Below
The "Showrunner" Delusion
Every ambitious healthcare leader shares a common, unspoken point of pride: If I’m not there, the place misses me. We wear our exhaustion like a badge of honor. We answer emails from the treadmill, solve interpersonal staff disputes on Sunday nights, and swoop in to patch up operational cracks before the patient ever notices. It feels like high-level leadership. It feels like being indispensable.
But let’s get honest: If your organization comes to a halt the moment you step away for four hours, you don’t own a sustainable business. You own a high-stress job where you are the primary bottleneck.
In clinical training, we are taught to obsess over the patient. But as an executive, founder, or clinical director, your primary patient is no longer the individual in the waiting room. Your patient is the organization itself. When your clinicians hit a wall, it is rarely a lack of commitment. It is a structural failure.
To heal the organization, you have to stop being the "Fixer" and start being the architect of a system that fixes itself.
1. The "Fixer" Trap and the 4-Hour Bottleneck
As a high achiever, your default setting is tactical execution. When a problem lands on your desk, your brain instantly fires up: How do I fix this? This instinct is a trap. Every time you step in to personally bridge the gap between faulty operations and a frustrated staff, you act as the organization's brakes. You absorb the friction, so the system doesn't have to change.
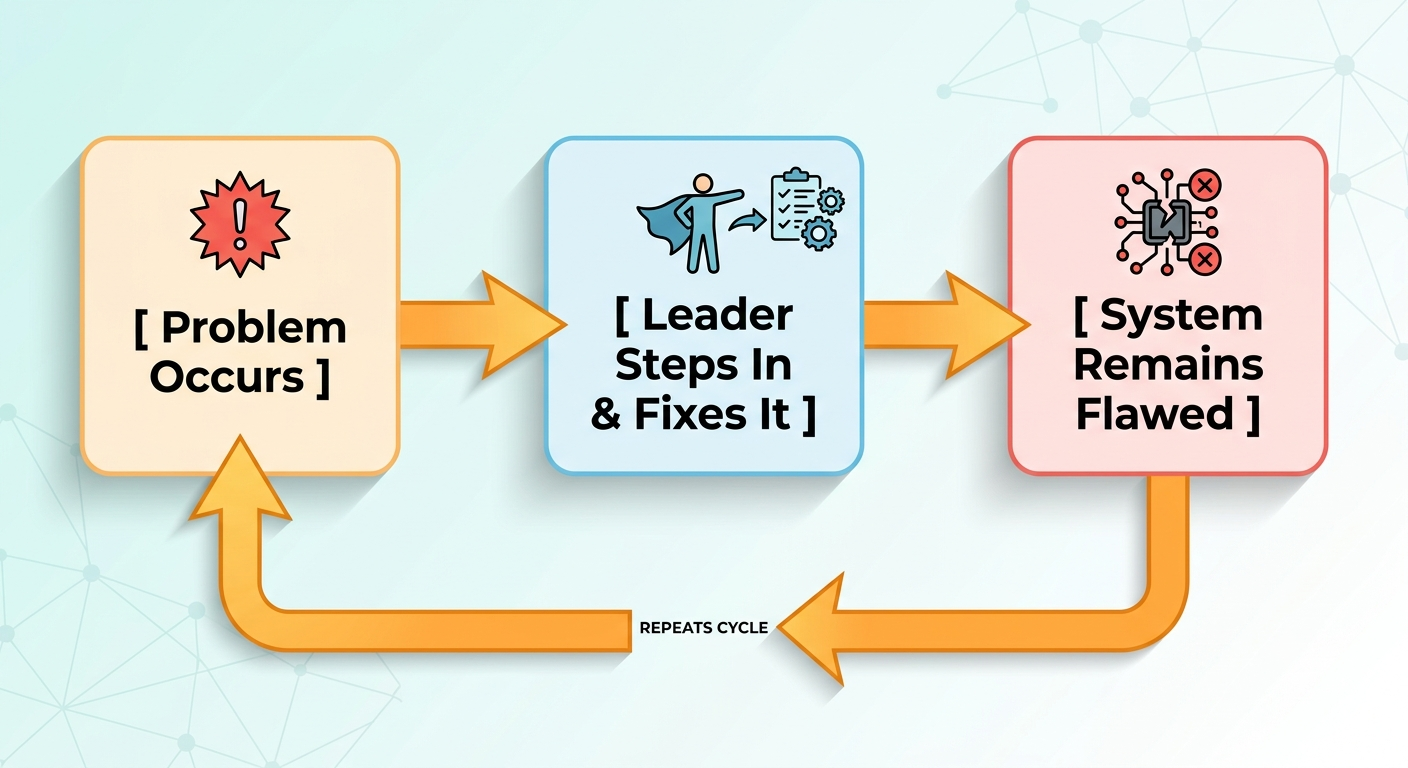
To break this cycle, you must consciously shift your internal dialogue. When an operational breakdown occurs, your first question cannot be How do I fix this? It must be: "What systemic guardrail is missing that allowed this problem to reach my desk in the first place?"
Recognizing the Gaps
Moving past the Fixer Trap requires identifying three distinct operational blind spots:
The Data Gap: Making reactive adjustments based entirely on your personal silo because you lack objective tracking on the ground.
The Solution Gap: Cultivating a culture where staff are trained only to bring you problems, rather than presenting data-backed resolutions.
The Capacity Gap: Becoming so buried in day-to-day firefighting that you completely abandon the strategic growth work you were actually hired to do.
2. Retention is a Structural Metric, Not a Personnel Problem
When turnover spikes, leadership teams routinely look out the window instead of in the mirror. We blame "the market," generational shifts, or salary competition. But passion doesn’t protect a clinician's nervous system from a broken culture. People rarely quit an organization's mission; they quit the daily friction that management allows to persist.
If you are trying to scale your practice or department right now, take a hard look at what you are building on top of. You cannot scale on the backs of a burnt-out team. Trying to hit growth targets by asking an over-capacity staff to "just push through" doesn't create expansion—it amplifies dysfunction.
Redefining Sustainability
True workforce sustainability requires auditing the elements of structural health that go beyond a paycheck:
The Pivot Rate: Do your clinicians have a clear, psychologically safe protocol to signal when they are at capacity, or is the unspoken expectation to just shoulder the load?
Invisible Labor: Are your women or clinicians of color carrying an unmeasured, uncompensated load of "emotional labor" or "culture building" without designated time-blocks in their schedules?
Clinical Agency: Do your providers have an actual voice in shaping their schedules and caseload complexity, or are they treated as interchangeable units of production?
3. The Perspective Gap: Who Was Your System Built For?
Setting the operational tone for an organization is a privilege, but it comes with a dangerous side effect: Default Bias. If you aren’t deeply intentional, you will instinctively build a system that only works seamlessly for people who move through the world exactly like you do.
This isn't an exercise in checking a corporate diversity box; it is an issue of cold, hard operational awareness. If you are a white, cisgender, able-bodied, or faith-based leader, your "standard" operating procedures may be creating invisible barriers for your team.
Operational Reality Check: You aren’t responsible for managing your employees' personal lives. However, you are entirely responsible for the equity of the environment they step into.
When a team member struggles to fit into a rigid, homogenous mold, that tension is rarely a "performance issue." More often, it's a perspective gap. If your systems refuse to acknowledge the real-world systemic hurdles your staff faces outside your walls—whether that looks like racism, gender bias, or socioeconomic barriers—you aren't leading. You are slowly excluding your best talent and accepting a higher turnover rate as a cost of doing business.
4. The "Gag Test": When Core Values Become Lip Service
We have all walked into clinics or corporate offices where phrases like "Patient-Centered Care" or "Inclusive Community" are proudly plastered across the walls. And we have all seen the collective eye-roll from staff when leadership actually invokes those words.
This is the Integrity Gap: the distance between your Aspirational Values (who you want to be) and your Operational Reality (what your systems actually reward).
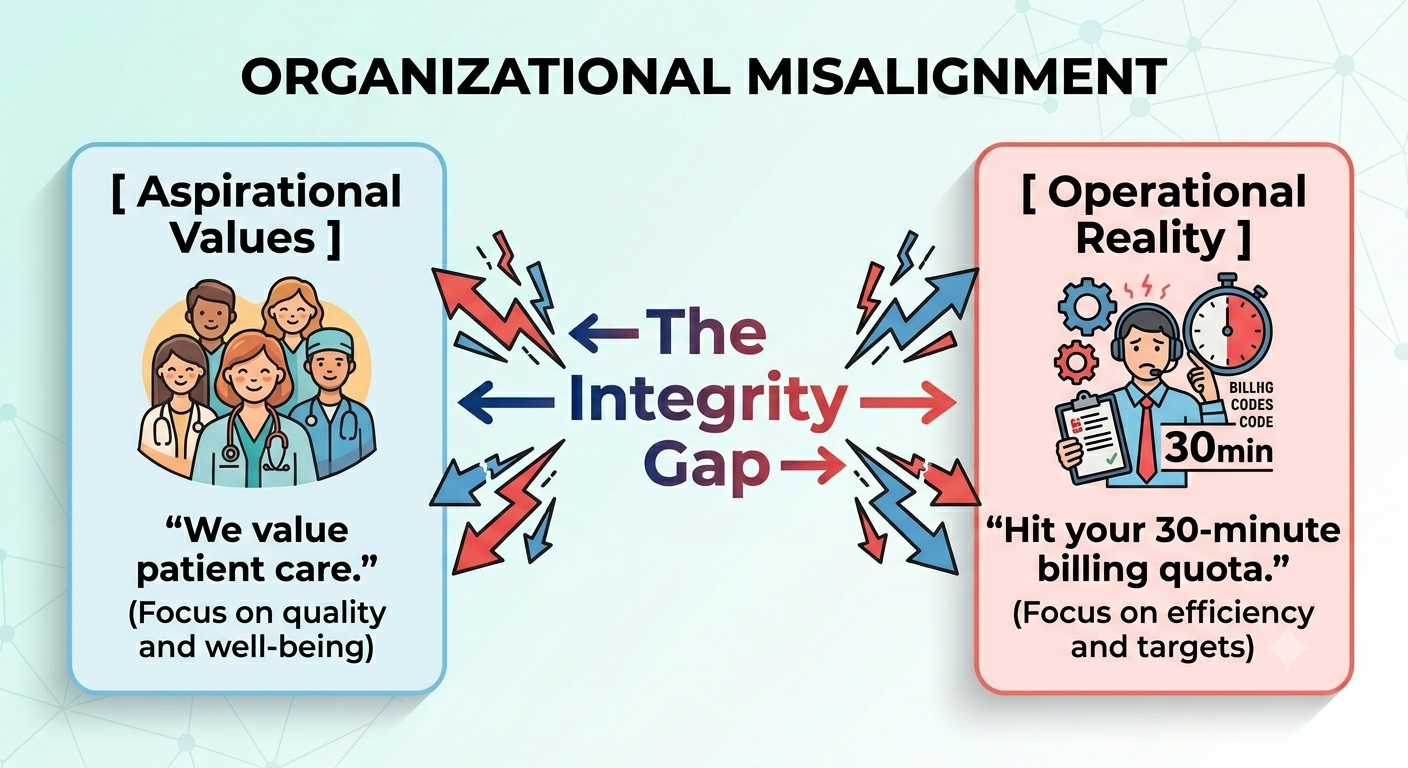
If your mission statement preaches unhurried, high-quality patient care, but your financial systems enforce back-to-back productivity quotas that leave clinicians no time to breathe, your system is a lie. Your team doesn't judge your values by your website copy; they judge them by what you reward, what you tolerate, and what you measure.
To close the gap, stop rewriting your mission statement. Start rewiring your operations. Restructure your metrics so that staying balanced, providing equitable care, and honoring boundaries are functional realities, not just polite suggestions.
Conclusion: Build the Machine That Fixes Itself
True leadership isn't about being the hero who saves the day; it’s about building a machine so resilient, clear, and equitable that it no longer needs saving.
If you want to transition from a chaotic, reactive environment to a proactive, sustainable organization, you have to start tracking the invisible friction points holding your team back.
Ready to run a diagnostic on your own practice? We’ve put together a comprehensive, no-nonsense tool to help you uncover your operational blind spots. Download our Systems-First Audit Checklist below to test your clinical workflows, calculate your true documentation burden, and uncover the structural gaps keeping you trapped in the "Fixer" loop.